This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 58 y old female resident of narketpally housewife by occupation came to opd
Chief complaints:
Abdominal distension since 10 days
Shortness of breath since 7 days
Pedal edema since 7 days
HOPI:
Patient was apparently asymptomatic 10 days back
Then she developed pain in the thighs for which she visited our hospital and took medication for that.
And then she developed abdominal distension which was insidious in onset and gradually progressive.
Abdominal tightness is present which is aggrevating after taking food.
She also had shortness of breath which is insidious in onset and gradually progessed to grade 3.
Patient also complained that she is gasping for breath after having meals so she even stopped having food properly.
Pedal edema is present since a week
Which is continuous , bilateral,pitting type and upto the knee level.
Past history:
She is known case of hypertension since 15 years and is on Tab. Telma 40 mg
Known case of hypothyroidism since 15 years and is on tab Tab.thyronorm
Known case of diabetes since 4 yrs and is on Tab.metformin 500mg
11 months back she was admitted in our hospital with similar complaints of abdominal distension,pedal edema and shortness of breath and after examination and investigations was diagnosed as Non alcoholic fatty liver disease.
Had 2 therapeutic ascitic taps done for symptomatic relief and was on medication since then .
She was having her routine monthly checkups since then
Since this 11 months patient had episodes of on and off pedal edema
Also complained of itching of skin all over the body which aggrevated on the days when she was constipated and also unable to pass the urine.
Now (6/7/23) Ascitic tap for done for diagnostic and therapeutic purpose and 600 ml of ascitic fluid was taken

Personal history:
She was married 38 yrs back has 2 children . Elder one is 36 old male married and younger one is 34 yrs old male unmarried. She is housewife does regular household work but due to complaints of sob, abdominal distension and swelling in legs she is unable to do her regular household work since 11 months .
Mixed diet
Appetite normal
Bladder movements-regular
Bowel - constipation (using Syrup:Lactulose )
Sleep - inadequate due to itching she couldn’t sleep properly
Addictions
Intake of beetle nut (pan) since 30 years
Daily routine :
Before 11 months:
She used to wake up at 5:00 am in the morning and get freshenup and do her regular house hold work of washing utensils , cleaning house,washing clothes and cooking upto around 9 am and then had her breakfast and used to watch Tv and then at 1 pm used to have her lunch and again household work at evng for 2-3 hrs and then has her dinner at around 9 pm and then used to go to rest .
Since 11 months:
She is unable to do any household work and just stays idle at home and even her appetite got reduced because of her distended abdomen .
Family history: No significant family history
General examination:
Patient was consious, coherrent and co-operative. Well oriented to time place and person.moderately built and nourished
Icterus -present

B/L pedal edema-present (upto knee level-pitting)

No pallor,cyanosis,clubbing,lymphadenopathy
Blackish pigmentation

Vitals:
Temp: afebrile
Bp: 100/70 mmHg
PR: 72bpm
RR: 20 cpm
SpO2: 98% on RA
Systemic examination
Per abdomen:
Abdomen - distended
Normal hernial orifices
Shifting dullness present
Dilated veins absent
No tenderness
No palpable mass
No organomegaly
No bruit heard


CVS:
S1 S2 heard ,No murmurs
Respiratory system:
B/l symmetrical chest
Trachea - Central
B/l air entry present
NVBS heard
CNS:
No focal neurological deficits
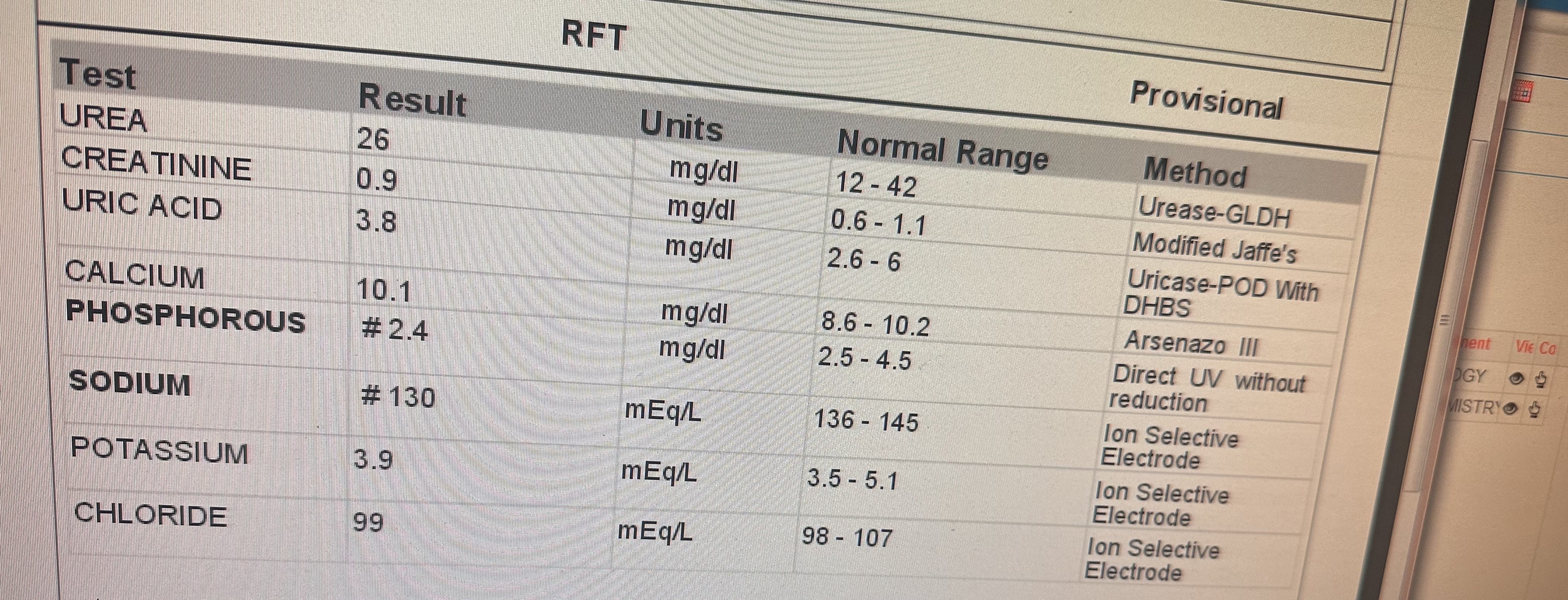
Investigations:









USG


DIAGNOSIS :
Decompensated chronic liver disease ?NAFLD with k/c/o HTN and hypothyroidism since 15 yrs
K/c/o DM-II since 4 yrs
Treatment :
1.Fluid restriction <1L per day
2.salt restriction <2g/day
3.tab.udiliv 300mg PO/BD
4.tab.rifagut 550mg PO/BD
5.tab.lasilactone 20/5mg PO/OD
6.Syp.lactulose 10ml PO/TID
7.syp.hepumerz 10ml/PO/BD
8.tab.telma 40mg PO/OD
9.tab.metformin 500mg PO/OD
10.tab.thyronorm 25mcg PO/OD
11.inj.vit K IV/OD for 3 days
12.high Protien diet -2 egg whites/day
13.strict I/O charting
14.weight and abdominal girth monitoring
15.monitor vitals
Comments
Post a Comment